

Shoulder impingement syndrome: causes, symptoms, diagnosis and treatment of shoulder joint pain caused by impingement
Shoulder impingement syndrome, also known as shoulder impingement syndrome, is a common cause of shoulder pain. It develops due to constriction in the shoulder joint, particularly in the space beneath the acromion, which can lead to irritation and inflammation of the tendons and bursae located there.
Diagnosis of shoulder impingement syndrome is crucial to initiate proper treatment and restore shoulder mobility.

Causes of impingement syndrome
Shoulder impingement syndrome can have various causes, often occurring in combination. These causes can be roughly divided into anatomical factors, overload and injury, and aging processes.
It is important to identify the exact cause of impingement syndrome in order to initiate targeted treatment. The symptoms of shoulder impingement syndrome can vary depending on the extent of the impingement and the resulting inflammation.
Anatomical factors
Anatomical variations in the shoulder joint can increase the risk of impingement syndrome. A common cause is the shape of the acromion, the bony projection of the shoulder blade that forms the acromion.
A hooked acromion can reduce the space below the acromion, the subacromial space, and thus cause constriction of the rotator cuff tendons. Bony growths or spurs in the shoulder joint area can also contribute to impingement and impair mobility. In impingement syndrome, the space below the acromion is often narrowed.
Overload and injuries
Repetitive overhead movements, such as those associated with overhead work or certain sports, can lead to strain on the rotator cuff tendons and the bursa below the acromion. This strain can cause inflammation, which further narrows the space in the shoulder joint and thus contributes to shoulder impingement.
Even acute injuries, such as a fall on the shoulder, can lead to inflammation and swelling in the shoulder joint, thus triggering impingement syndrome. Treatment for impingement syndrome should reduce inflammation.
Aging processes
With increasing age, degenerative changes can occur in the shoulder joint. These include, for example, wear and tear on the rotator cuff tendons, which can make them more susceptible to injury and inflammation.
The formation of bone spurs on the acromion, the roof of the shoulder, is also a common phenomenon in the aging process and can reduce the space below the acromion, increasing the risk of subacromial impingement. These changes can lead to shoulder pain and limit shoulder mobility. Discomfort may occur when raising the arm laterally.
Typical symptoms of impingement syndrome
Pain in the shoulder joint
The main symptom of shoulder impingement syndrome is pain. This shoulder pain may begin insidiously and gradually worsen, or it may occur suddenly following an overhead movement or injury.
The pain is often movement-dependent and occurs particularly when raising the arm to the side or during overhead movements. The pain from impingement can also be present at rest, especially at night, and disrupts the patient's sleep. The pain often radiates into the upper arm and can extend into the elbow.
Restriction of mobility
In addition to pain, the syndrome often leads to limited shoulder mobility. Those affected have difficulty fully raising their arm or moving it behind their back. These movement restrictions are caused by the pain and inflammation in the joint.
Impingement can lead to a protective posture, which further reduces mobility. In advanced stages, impingement can even lead to frozen shoulder, a complete stiffening of the shoulder joint. Timely treatment can restore shoulder flexibility.
Pain radiating into the arm
Another typical symptom of impingement syndrome is pain radiating into the arm. The pain can radiate from the glenohumeral joint into the upper arm, elbow, and even the hand.
The radiating pain is often caused by nerve irritation in the shoulder area, which occurs due to the irritation and compression of impingement. Shoulder pain can also be described as dull, stabbing, or burning. These symptoms can significantly impair the patient's quality of life.
Treatment for impingement syndrome aims to relieve pain.

Diagnosis of impingement syndrome
Clinical examination
Diagnosis of shoulder impingement typically begins with a thorough clinical examination by a physician or physiotherapist. This includes testing the shoulder's range of motion and palpating for painful areas.
Special tests, such as the Neer test or the Hawkins test, can be performed to provoke the impingement and confirm the diagnosis. The doctor will also ask about the patient's medical history to identify possible causes of the impingement, such as overhead work or injuries.
The clinical examination is crucial for further therapy.
Imaging techniques
In addition to the clinical examination, imaging techniques can be used to confirm the diagnosis of shoulder impingement syndrome and to rule out other causes of shoulder pain.
For example, X-rays can show bony changes, such as bone spurs on the acromion, that contribute to impingement.
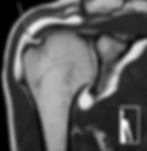
Magnetic resonance imaging (MRI) can evaluate soft tissues, such as the rotator cuff tendons and bursa, and reveal inflammation or tears in the tendons. Ultrasound examinations can also be used to evaluate the tendons and bursa.
The diagnosis of impingement is relevant for treatment.

Treatment options for shoulder impingement syndrome
Conservative therapeutic approaches for impingement syndrome
Conservative treatment of shoulder impingement syndrome focuses on relieving shoulder pain and restoring mobility. This includes various measures such as the administration of painkillers and anti-inflammatory medications, such as cortisone, to relieve irritation of the bursa (bursitis) under the acromion.
Physical therapies such as heat or cold applications are also used to relieve the pain of impingement syndrome. These conservative treatment approaches are often the first choice for treating impingement syndrome before considering surgery and aim to improve symptoms and restore shoulder function.
Physiotherapy
Physiotherapy is an essential component of treating impingement syndrome. Targeted exercises are designed to improve the shoulder's range of motion and strengthen the muscles surrounding the joint.
Physiotherapy treatment often includes manual therapy to mobilize the joint capsule and release adhesions. An important aspect is learning exercises that patients can perform independently at home to maintain long-term shoulder mobility and prevent recurrence of impingement.
Physiotherapy helps reduce the symptoms of shoulder impingement syndrome and improve the function of the affected shoulder. Therapy contributes to reducing the strain on the tendons.

Surgical treatment of impingement syndrome
If conservative treatment approaches do not provide sufficient relief for shoulder impingement syndrome, surgery may be considered.
The goal of the operation is to expand the space under the acromion to relieve the compression of the rotator cuff tendons. This can be achieved through arthroscopic surgery, in which bone spurs on the acromion are removed and inflamed tissue is removed. In some cases, the bursa may also need to be removed.
The surgery is intended to relieve shoulder pain and restore shoulder flexibility.
The decision for surgical treatment should always be made in consultation with the treating orthopedist.

Therapy and aftercare for shoulder impingement syndrome by orthopedists
Rehabilitation after impingement syndrome
Regardless of whether shoulder impingement syndrome is treated conservatively or surgically, rehabilitation plays a crucial role in treatment success. After surgery, intensive physical therapy is required to restore shoulder mobility and strengthen the muscles.
Even after conservative treatment, physiotherapy exercises can help stabilize the shoulder and prevent recurrence of impingement. It is important that the patient actively participates in rehabilitation and performs the exercises regularly.
Consistent follow-up care can alleviate long-term discomfort and optimize the function of the shoulder joint.
Long-term prevention of impingement
To prevent a recurrence of shoulder impingement syndrome, long-term preventive measures are important. These include various aspects, such as:
Avoiding overhead work and overhead movements that place strain on the shoulder joint.
Regularly stretch and strengthen the shoulder muscles to stabilize the shoulder and prevent impingement.
Good posture and ergonomic workplace design can also help reduce strain on the shoulder. At the first signs of shoulder pain, you should consult a doctor or physiotherapist early to initiate timely treatment and prevent the progression of impingement syndrome.
The treatment of impingement syndrome aims to preserve shoulder mobility.
👉 Make an appointment now – we will advise you individually on your shoulder problem.

FAQs about impingement syndrome.
When is surgery necessary for impingement?
When pain does not subside despite physiotherapy and injections.
How is impingement operated on?
Usually arthroscopically by removing constrictions and smoothing the bursa.
What are the risks of surgery for impingement syndrome?
Inflammation, scarring, or recurrence of symptoms are the most common risks after surgery for impingement syndrome, but are overall very rare.
I'm having surgery for impingement syndrome. When can I go back to work?
Depending on the workload, you may be able to return to work after just a few days. During the first six weeks, the arm should not be abducted beyond 120° and should not be subjected to maximum strain; however, office work, for example, is usually possible after two weeks.
Sports after impingement surgery: When can I resume?
Many sporting activities can be resumed a few weeks after impingement surgery. Running, hiking, and cycling, in particular, can be resumed quickly. Overhead sports like tennis or certain fitness exercises can take some time to return to their previous level. Shoulder mobility is usually the culprit, as it is often limited after surgery. Specific exercises and targeted physical therapy can help ensure a quick return to sport.


PROF. DR. MED BEN OCKERT
Specialist in orthopedics and accident surgery, sports medicine.
